
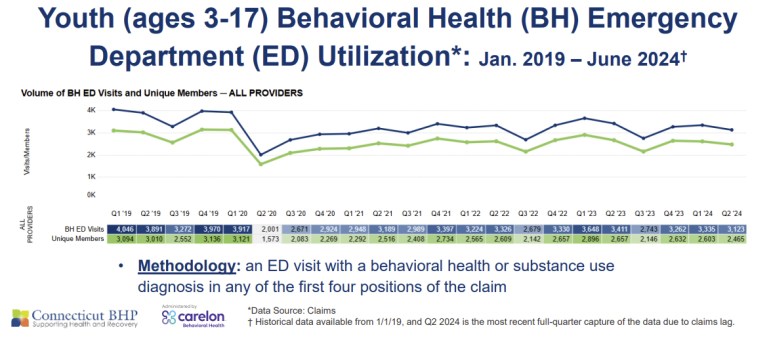
13,064. That’s the number of times children covered by HUSKY visited Connecticut emergency departments for behavioral health crises in 2023.
Suicidality, severe anxiety, major depression, self-harm. For anyone counting, that is a massive increase in behavioral health visits by Medicaid-covered children since the Hartford Courant ran a front page story on emergency room crowding in 2007. Thirteen thousand visits to EDs that are often crowded with other people in crisis; children in chairs, carrels, and even gurneys; parents anxiously watching the clock as the daylight hours turn to night.
This may feel familiar. That’s because every five years or so a spike of press coverage about children stuck in emergency rooms has pushed this issue to the front burner and spurred some modest policy improvements. Yet here we are again. And there they are: children with acute behavior health needs spending the night in the ED and parents reluctantly shuttling between home and hospital, praying for an answer to come the next day.
What’s going on here? Why are these key indicators of children’s behavioral health getting worse over time? And what do we need to do to make it better? I am encouraged by the work of the state’s new Transforming Children’s Behavioral Health Taskforce, which has recommended increased investment in children’s mental health services. Legislators will need to heed the TCB’s recommendation, but our state will need to do much more to meet our kids’ needs.
Having gone through this often and recently, Connecticut can learn some lessons about how to make things better:
We’ll get what we pay for. Chronic underinvestment in behavioral health has resulted in predictable waiting lists, labyrinthine paths to care, and decimated workforces. We need Medicaid rates that cover the actual cost of care; a reasonable and regular rate-setting structure, and a quality improvement structure to track progress in utilization and healthcare outcomes.
The state must have a strategy to ensure that services are equally available to all children, no matter how they are insured. Good models exist for this; we just have to implement them. Healthcare spending rules must be flexible enough so that money can be spent on a child’s whole family and address health-related social needs – where research says we get the most bang for our healthcare dollar. The state must have a strategic, monitored, and accountable plan for workforce development from high schools to vocational schools to colleges to licensing frameworks.
Improving treatment options won’t be enough. Behavioral health is tied to healthy development. There are not enough social workers or outpatient clinics in all the land to eliminate the stressors and anxieties our kids (and families) are reporting.
Children who are hungry or who have unstable housing or who can’t access afterschool activities because of a lack of familial resources or adequate transportation will spend their days worrying and reacting, not learning and thriving. Behavioral health starts with meeting children’s basic needs in the community and providing opportunities for them to flourish.
Connecticut must have a Children and Families Agenda. We must create a comprehensive vision for health, education, and wellness in this state (and in this country), and reject policies that lurch us from one spending cycle to the next.
State leadership is good at talking about out our generational vision for debt reduction, which is good! But we must bring that same energy to a generational plan for thriving communities—where every child in Connecticut is well-housed, well-educated, healthy, and engaged in meaningful community activity and relationships. This will not happen on its own, as we can see with deteriorating academic and mental health outcomes for our children. We must set out our north star and ensure that biennial budgets are moving us closer to our vision.
Every day in policy and politics we must ask ourselves, what kind of world do we want to build? Our policy, and indeed our core value as a state, should be that healthy thriving children are our priority, and we should be willing to invest in making that value a reality.
Over 13,000 trips to the Emergency Department for Connecticut children in crisis—our children. They are waiting for us to act.
Sarah Healy Eagan is Executive Director of the Center for Children’s Advocacy.
link